Treating Gingival Recession at Fulham Road Dental

The gingival margin is clinically represented by a scalloped line that follows the outline of the cemento-enamel junction. It is located 1-2mm coronal to it. Gingival recession is an apical shift of the gingival margin with exposure of the root surface to the oral cavity.
This mucogingival deformity has a complex multifactorial aetiology. In some individuals, gingival recession may be asymptomatic, however gingival recession can cause: dentine hypersensitivity, tooth abrasion, carious root lesions, non-carious cervical root lesions and aesthetic concerns.
Tissue related characteristics known to influence the extent of recession are :
- Keratinised tissue width
- Gingival thickness
- Bone morphotype
The term periodontal phenotype describes the combination of gingival phenotype (three-dimensional gingival volume) and bone morphotype ( the buccal bone plate thickness).
A commonly used method to measure gingival thickness during a basic periodontal examination involves inserting a periodontal probe into the gingival sulcus. In a thick phenotype, the probe is not visible, and the thickness is approximately ≥1mm, whereas in a thin phenotype the gingival margin is associated with more transparency. The visibility of the probe through the gingival margin suggests an associated thickness of ≤1mm. Thin gingival phenotypes have been described as being more prone to gingival recession.
The gingival phenotype can be changed as a result of both environmental and clinical intervention. Moreover, both gingival thickness and keratinised tissue widths can vary at different sites in the mouth.
Anatomical and pathological factors associated with gingival recession.
Tooth position
The bucco-lingual position and orientation of the tooth in the alveolar housing can influence the thickness of the overlying gingival tissues, and hence the amount of gingival recession present. Mandibular recession has been reported to be more frequently associated with post-orthodontic recession.
Plaque induced factors.
Bacterial plaque-induced gingival recession defects are caused by plaque accumulation localized to the buccal surface with no severe interdental attachment loss; thus, they can be successfully treated with root-coverage procedures. Patients with bacterial plaque-induced recessions must be shown how to perform optimal oral hygiene, and mucogingival surgery must not be performed until good plaque control has been achieved.
Periodontal disease and treatment of periodontal disease
In patients with periodontitis, bacterial plaque (specific periodontal pathogens) causes connective tissue attachment loss that may clinically manifest with gingival recession, not only at buccal surfaces but also at the interproximal tooth surfaces. Gingival recession can occur following both surgical and non-surgical periodontal treatment. Overall, there may be remodelling of the gingival margin resulting in an apical shift of the gingival margin.
Mechanical trauma
Toothbrushing is commonly associated with gingival recession and partly explains the correlation between low plaque levels found at sites of recession. Trauma can be caused by ‘traumatic toothbrushing’.
Clinical signs of gingival recession caused by toothbrushing are soft-tissue ulcers (without pain) and hard-tissue cervical abrasions (non-carious cervical lesions). The cervical abrasions are caused by continued mechanical trauma after recession manifestation. Sometimes, soft-tissue trauma may destroy all keratinized gingival tissue. Patient’s using a powered toothbrush should not use a scrubbing technique and some individuals may benefit from using a sensitive head with softer bristles. The presence of a traumatic brushing technique, in the presence of a predisposing factor such as thin periodontal phenotype, may make the patient more prone to developing gingival recession. Improper use of dental floss may also result in gingival recession. The initial injury may appear as an acutely inflamed, ulcerated linear or V-shaped cleft that is symptomatic. This can usually be assessed by asking the patient to demonstrate their flossing technique.
Lip or tongue piercing
Tongue piercing has been directly related to dental and gingival injuries on the lingual aspect of the anterior lower teeth. Buccal gingival recession may occur in subjects in whom the lip stud is located such that it can directly traumatize the gingival margin.
Removal partial dentures
Poorly designed and ill-fitting dentures can cause gingival recession of abutment teeth and increase pressure on supporting tissues.
Direct trauma from malocclusion
Some malocclusions, such as Class II Div. II are associated with a deep overbite and often a reduced overjet with retroclination of the upper anterior teeth. In some severe cases this can result in direct trauma to the labial gingiva of the lower anterior teeth or to the palatal marginal gingiva of the upper anterior teeth
Muscle attachments
Strong frenum attachments can also contribute to gingival recession (see figure 1).
Smoking
An increased prevalence of gingival recession has been shown in those who smoke or use smokeless tobacco products.
Diagnosis of recession defects
Assessing the clinical and radiographic aspects of gingival recession, to facilitate treatment planning are key to achieving successful and predictable treatment outcomes. During a basic periodontal examination, a periodontal probe can be used to measure the distance between the gingival margin and cemento-enamel junction. This can be done at three points on the buccal surface and three points on the lingual surface. Baseline photographs, digital scans and dated study models can be useful aids to monitor gingival recession over time.
In 2017, a new treatment orientated classification was proposed by the combined EFP and AAP 2017 World Workshop. This replaced the previous classification described by Miller.
| Recession Type 1(RT1) | Gingival recession with no loss of interproximal attachment. Interproximal CEJ is clinically not detectable at both mesial and distal aspects of the tooth |
| Recession Type 2 (RT2) | Gingival recession associated with loss of interproximal attachment. The amount of interproximal attachment loss is less than or equal to the buccal attachment loss. |
| Recession Type 3 (RT3) | Gingival recession associated with loss of interproximal attachment. The amount of interproximal attachment loss is greater than the buccal attachment loss. |
Table 1. Recession type classification proposed by the 2017 World Workshop.

Figure 1. Example of RT1 recession on tooth position 31. Note the reduced keratinised tissue width and prominent frenum attachments.
Surgical management of gingival recession
Gingival recession can be treated with various surgical procedures. Recognising the aetiological factors contributing to gingival recession is key to managing gingival recession defects. Periodontal phenotype is difficult to modify without performing surgery, however tooth position can be corrected with orthodontic therapy. A referral to an orthodontist can be considered. Furthermore, providing good oral hygiene advice to the patient to promote an atraumatic toothbrushing technique and optimal oral hygiene methods are vital.
Coronally Advanced Flap with connective tissue graft
This method is commonly used to achieve total root coverage in isolated and multiple recession sites. This method requires harvesting a connective tissue graft from the palate. This graft is then sutured onto the defect, and it is subsequently covered by a coronally advanced flap.
a)
b)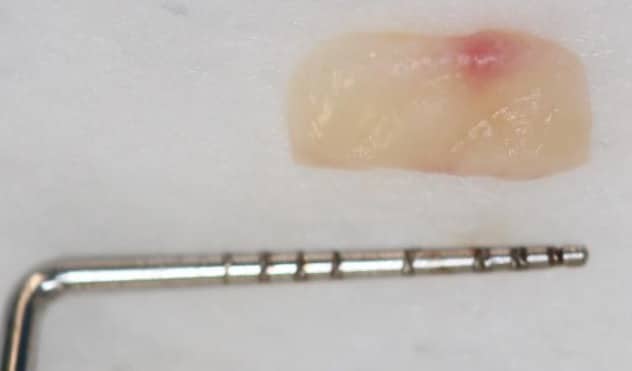
c)
d)
e)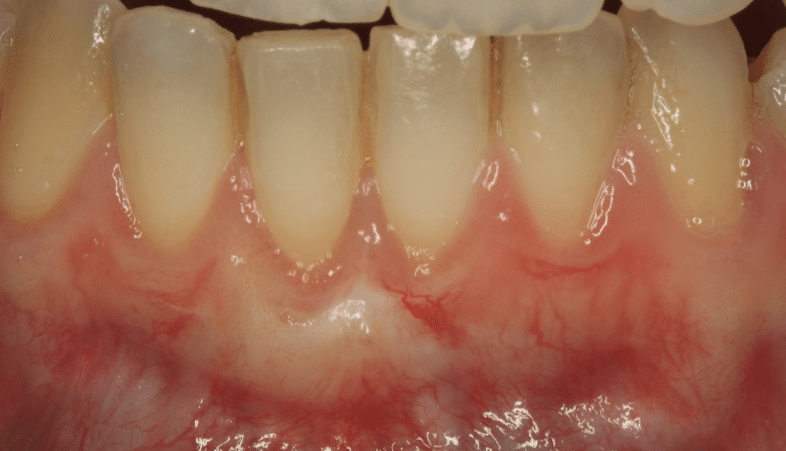
Figure 2. Surgical management of lower anterior recession using a coronally advanced flap and subepithelial connective tissue graft.
Free gingival grafts
This surgical technique first described by Bjorn 1963, and later modified by Sullivan and Atkins in 1968, is commonly used for mandibular recessions where aesthetic concerns are of less importance. The colour match to the surrounding gingival tissue is unpredictable, however this method is a predictable surgical technique to primarily increase keratinised tissue width. Some root coverage may be achieved. Over time a ‘creeping attachment mechanism’ can occur. This attachment results in the post-operative migration of the free gingival graft in a coronal direction, thereby increasing root coverage over time. Both surgical techniques can also be used around implants.

Figure 3. An epithelialised free gingival graft to increase keratinised tissue width.
There are many other surgical techniques, such as tunnelling, which can be used with or without a subepithelial connective tissue graft.
Frequently asked questions by patients and dentists:
‘’ Will my recession get worse?’’
A systematic review by Chambrone in 2016 evaluated the long-term outcomes of untreated buccal recessions defects. The results showed limited but consistent evidence that untreated buccal GR defects in individuals with good oral hygiene were highly likely (78% of defects) to progress. Individuals experienced an increase in recession depth during long-term follow-up. The decision whether or not to treat a recession defect should be judged on an individual basis after a detailed periodontal examination.
‘’ Will recession cause tooth loss?’
Recession associated with untreated periodontitis can result in tooth loss, however recession due to the other aetiological factors will not generally cause tooth loss.
‘’When do I refer patients with gingival recession?’’
If gingival recession is noted by the general dental practitioner during a dental examination or a hygienist during hygiene treatment, it can be monitored using the methods previously described. If the gingival recession deteriorates or if the patient presents with dentine hypersensitivity, difficulty maintaining good oral hygiene or has specific aesthetic concerns, a specialist referral should be considered. The management of the recession defect will depend on several factors including the anatomy around the defect, and aesthetic demands, both of which will influence the choice of technique.